I’ve always been a fan of the “go with the flow” outlook on life, and my diagnosis did not change that. Sure, I see more needles in a day than most people my age see in a year, but that doesn’t stop me from doing the things I love.
Yes, there are challenges, but it takes more than a faulty pancreas to stop me. I still surf, skate, go out, and love my life.
It’s safe to say that being diagnosed with type 1 diabetes (T1D) was the hardest hit I’ve taken in my life. T1D threw me and my family for a loop, and although life would be easier without it, this disease has opened me up to new experiences that I never would have had before my diagnosis. The most important of these new experiences is undoubtedly my Diabetes Alert Dog (DAD), Annabelle. She is my furry shadow, my best friend, and I can’t see my life without her.
I had experience with alert dogs even before my diagnosis—My mom, Becky Causey, is president of the Diabetes Alert Dog Alliance— and even before that I had several dogs in the house while I was growing up. It only made sense that I would get an alert dog. Now, almost 4 years later, I can’t even fathom not having a DAD. Annabelle follows me around the house and out in public like she and I are attached at the hip. When I don’t have her beside me, it’s the same feeling as if I forgot my phone.
Mac’s experience with alert dogs, although different and more intimate than most, is not entirely unique. In an mlive article, a 13-year-old Grand Blanc student named Joseph talks about Pepsi, his Labradoodle and Diabetes Alert Dog. Pepsi goes everywhere with Joseph, including basketball games, friends’ birthday parties, and especially during the nighttime hours when blood glucose levels often dip dangerously low.
Jedi, a Labrador, is another Diabetes Alert Dog who takes care of an 8-year-old boy named Luke. In an article by the Huffington Post, the miraculous experience of Jedi saving Luke’s life is explained. In the middle of the night, Luke’s levels dropped extremely low, and as he was trained to do, Jedi woke Luke’s parents to let them know.
These stories are just a few examples of the profound impact that a Diabetes Alert Dog can make on a person’s life. This impact comes in many forms, particularly in their ability to recognize when the person is in danger, but also the companionship, love and support that service dogs and pets provide us.
This article reports on survey responses from young adults with type 1 diabetes in New Zealand. The survey asked them about their thoughts on what they would like from a mobile phone app to help manage their diabetes. They found that these young adults would like an app that gives them:
Tips on taking care of their diabetes,
Motivational messages,
Reminders to test their glucose
My Biggest Takeaway
Honestly, my biggest takeaway is that we are developing our app (MyT1D Hero) with all the right things in mind! This article provides further proof that young people have mobile phones and are likely to use them to help them take care of their diabetes.
My Concerns on the Article
The authors state some limitations in the article about the size of the study, but a lot of the news surrounding this article makes it seem like this was a larger study. They invited 402 people to take the survey, yet only had 115 responses. That is a bit low. Also, these are young people from New Zealand, who may not be representative of young adults in America (or other countries).
I also have some concerns on how the ideas were presented. It is one thing to say, “How much would you like to get a motivational message?” It’s completely different to actually have people receive the messages, and then ask them their thoughts on the messages.
They also did not ask (or report) about any support person(s) and how well they are currently managing their diabetes. For example, parents of kids with type 1, like we are researching.
Overall
This is a fairly short, well-written piece, which provides additional evidence for our current app development.
By: Amanda Holmstrom, PhD, Associate Professor of Communication, Michigan State University
We often hear that “emotional support” is important for people with chronic conditions like type 1 diabetes. However, what is emotional support? How can we be sure to provide good emotional support to our loved ones?
Amanda Holmstrom, PhD.
Emotional support is care and concern shown toward someone who is having a tough time. For example, you might want to cheer up a friend who’s upset because she’s having difficulty managing her blood sugar. Or, you might want to comfort your child who’s hurting after a classmate made a nasty remark about him missing a lot of school for doctor’s appointments.
Research shows that providing and receiving emotional support is an important component of our close relationships. However, there are so many ways that we could help our loved ones when they are hurting that it’s easy to get confused about what to do. We really want to help, but sometimes we end up having the opposite effect.
Fortunately, a lot of research has been done to help us know how to help others when they need emotional support. Here are some research-approved strategies that are usually seen as helpful:
Find a time and place: Make sure that you have the time to talk and an appropriate place to do so. For example, it’s hard to offer really good emotional support in the 20 seconds before your child runs out the door to catch the bus. Carve out some time where the two of you can feel free to say what’s on your minds.
Say you care and want to help. Make sure to tell your loved one directly that you care about her and that you are available and willing to help. For example, you could say, “I love you, and I want the best for you. I want to help you in any way I can.”
Ask what’s going on. Ask your loved one to talk about the situation and how he is feeling. A simple, “What’s troubling you?” will often get the ball rolling.
Legitimize feelings. Let your loved one know that you understand how he feels and that his feelings are perfectly normal. For example, you could say, “I can see you’re upset, and it makes a lot of sense that you’d feel that way.”
Use eye contact and body language to show care and concern. For example, you could nod to show that you’re listening or offer a hug to show you care. Oftentimes the most helpful thing we can say isn’t said with words.
On the flip side, some of the things we often do to provide emotional support are generally seen as unhelpful. Here are some things to avoid:
Don’t offer unsolicited advice. The most common error people make when attempting to provide emotional support is to offer unwanted advice. We tend to do this because we want to fix problems, but research shows that unless someone asks for advice, it’s often best not to offer it.
Don’t downplay feelings. Denying, ignoring, or criticizing your loved one’s feelings is generally hurtful. For example, resist the urge to say something like, “It’s not a big deal” or “You don’t need to be so upset!”
Don’t overdo it. Though it’s important to show your loved one that you care, try not to be too over-the-top in your concern. Give him room to breathe and process things on his own, too.
Though it’s not always easy to provide, emotional support is consistently rated as one of the most important components of our close relationships. By giving your loved ones good emotional support when they need it, you not only help them, but you keep your relationship strong.
Dr. Bree Holtz’s summary of the article, Management of Children with Diabetes in the School Setting
Article Overview
This journal article is about the role of diabetes educators when there is a child with diabetes in school. The article is a position piece of the American Academy of Diabetes Educators. While the article does mention type 2 diabetes management and other types of diabetes, this article seems to be generally focused on management of type 1.
My biggest takeaway
It offers a description of what a diabetes educator does and the role they can take when trying to navigate care of a child in the school setting. This is the part of the article that I thought might be the most helpful for parents to know. From the, admittedly very few parents I have talked to, I’m not sure that people are using diabetes educators in this way. The article says that a diabetes educator can (p.35, direct quote):
Be the primary contact and liaison between the school, parent/guardian, and diabetes health care team
Be a resource for training and educating the school nurse and school personnel in the care of students with diabetes
Educate and facilitate behavior change of students with diabetes, parents/guardians, and school personnel
Provide resources and expertise to help develop, implement, and update the written school-based diabetes medical management plan (DMMP)
Other key points
The paper then briefly describes:
laws surrounding care for students with diabetes;
plans for diabetes management
They also go on to describe how the American Association of Diabetes Educators (AADE) 7 Self-Care Behaviors can be applied to the school setting. This is something that they are really promoting throughout the profession and it is called AADE7 for short. These behaviors include:
Healthy Eating
Being Active
Monitoring
Taking Medication
Problem Solving
Health Coping
Reducing Risks
They then provide a list of additional resources that could be helpful to parents.
Reference:
AADE (2017). Management of Children with Diabetes in the School Settings, The Diabetes Educator, 43: 36-39.
*Note: if you would like access to the full article, please request by article title via email to (murra172@msu.edu).
By Reece Ohmer, high school sophomore living with T1D since 2009
With Valentine’s Day quickly approaching, I thought I’d share my opinion about the holiday of love.
I have been living with T1D since I was eight years old, and I can’t remember a time when I didn’t have to constantly check my blood sugar levels, monitor my food intake, and set the correct dosage of insulin.
Reece Ohmer, now a high schooler
With that being said, I vividly remember every Valentine’s Day as a child. I grew up in a household that believed in the saying ‘kid first, diabetes second’ and this has truly become the mantra of my life.
Valentine’s Day was no exception. I was able to enjoy all the festivities and parties (as well as yummy treats) that any other kid living without T1D was able to partake in. I do remember my mom and Miss Dawn, my school aide, buzzing around but only to make sure that I was treated equally in every regard. The kid that got the chocolate lollipop coated in extra sugar balls? Yes, there was one for me too.
Reece in elementary school
The funny thing about parties in elementary school is that they all revolved around food, specifically pizza. I remember having to pay extra attention to my BGs on these days, but even still, I enjoyed that gross, greasy cheese pizza with all the other kids. It may not have been good but I did it anyway- mostly because I could.
During the party, you were also allowed to pass out Valentine’s to the class, just as long as every child received one. Most of these Valentine’s consisted of an attached candy or food item. To be different, I always passed out cool, non-food Valentine’s to the class. I remember getting all this candy and not eating any of it. Not because I couldn’t eat it, but just the fact that I had the sweets in my possession was enough to make me smile. Ironically, the kids that received my Valentine’s felt special to get something that wasn’t super generic. One year, I passed out miniature bottles of bubbles. In minutes, the room looked magical with little tiny bubbles floating around the classroom. I felt like a rock star.
Reece has been living with T1D since 2009. She truly is a T1D Hero!
Looking back at my elementary days, as I am now in high school, I realized that I don’t remember the specific food or the candy that was given during the parties, I only remember the fun activities the class did together or the new adventure that my classmates explored.
It’s a bit ironic that our school created a holiday that revolved around eating, when in reality the only thing I remember from Valentine’s Day as a kid is the crafts we made and the party the class had. For me, Valentine’s Day was about playing games and being with the people you really cared about. I’m certain that I will carry that feeling of love and friendship throughout life.
Life with diabetes presents many challenges and stressors. In the beginning, after moving past the shock and grief of diagnosis, the biggest challenge becomes learning the basic skills of diabetes caregiving.
These include: carb counting and providing a consistent meal plan every day; measuring
blood glucose levels at meals and prior to bedtime, as well as when one feels low; and proper use of mealtime and nightly insulin.
Julie Dunneback
Learning how to take care of diabetes during times of sickness is also important, as is learning how to take care of diabetes during recess, gym class, basketball season, or vacations.
One must take these skills out into the real world of school or work and life with friends and family. Unfortunately, no one can fully understand what it is like to battle diabetes unless you are the person living with it, on that particular day, in that particular moment.
Diabetes affects the here and now, but also complicates each developmental milestone that a person with diabetes reaches.
Many good intentioned people offer suggestions, whether from other persons with T1D, parents of other kids with diabetes, teachers and counselors, or health care providers.
While these tips can be helpful, they may not necessarily be accepted.
The person with diabetes does not always want help or the solution that is offered. They may simply want someone to listen and to understand their experience.
Individuals often want someone to stand with them during times of stress, to listen, and to act as a supportive friend. Provision of love and acceptance is often more helpful than giving unsolicited advice.
With that in mind, please consider these diabetes dos and don’ts when interacting with persons with diabetes:
Offer a listening ear, not judgmental comments or unwanted advice.
Make no comment about dietary choices. Don’t ask if the person with diabetes can eat what everybody else is eating.
Allow for privacy, if desired, or at the very least, do not call attention to blood glucose testing, injections or dosing if the person with T1D is using an insulin pump.
Treat the person with T1D like any other friend or teammate; do not single them out because of their diabetes.
Above all, see them as an individual, not as someone with an illness or a disease.
Julie in her clinic
While these guidelines are often helpful, it is imperative to assist a person with T1D if they are ill, confused, or otherwise unable to assist themselves.
Most importantly, remember to take it one day at a time, especially when the burden is great, whether you are the caregiver or the person living with diabetes.
Daily diabetes care is hard work, and it’s ok to have an off day, just do not give up on yourself if the choices have not turned out well that day, start fresh the next day. Accept your best efforts each day as enough.
Disneyland Paris… the place where dreams are supposed to come true. But it was here in 2002, aged 16, that I collapsed, fell unconscious and had to be airlifted to hospital, where I almost died.
Laura Cleverley has conquered her diabetes (Photo: Sunday Mirror)
I was diagnosed with Type 1 diabetes and faced living with a long-term condition involving multiple daily injections, finger pricks and much more.
France is where I was taught to inject insulin, in a language that I didn’t speak, and spent what seemed like hours with a needle hovering over my leg as tears poured down my face, wishing the nightmare away.
That day signaled 10 years of self-neglect as I desperately tried to hide from my condition.
Initially I was frightened, angry and confused and the information that I was provided with in order to manage my diabetes was sparse and outdated.
Laura Cleverley has dealt with her diabetes (Photo: Sunday Mirror)
When you get a diagnosis of a long-term condition, some form of education is incredibly important – but it was something I was not provided with.
For years I did not understand the condition that caused me to feel so unwell; I lacked even the basic knowledge and looking back I wish I’d had the courage to stop and ask, not just accept that what I was being told was correct.
At the time I did not know that my pancreas was still producing a small amount of insulin and the large amount of insulin I was advised to take was causing my glucose levels to become dangerously low.
This, combined with the stigma that was associated with injecting, is what caused me to stop taking my insulin and I soon became very unwell.
I received comments from friends such as, “Do you have to inject in front of us?” and, “I don’t know how you can do that to yourself”.
The 16-year-old me was incredibly self-conscious about what people thought and I was desperate to fit in with my peers.
The fact that I was taking life-saving medication should have been my priority and I deeply regret not standing up for myself at the time.
Each day became an ever-worsening battle to muster the energy to move, think, even to smile as my glucose levels became higher, but I carried on regardless because I didn’t know what else to do.
Insulin injection (Photo: Getty)
I had become so disengaged from my healthcare team that I felt I had nowhere to turn. I soon became an expert at hiding the symptoms caused by missing insulin injections.
I would lie to my family and tell them that I was taking my insulin as required; I could feel the strain that diabetes was having on me and I couldn’t bear the thought of my family suffering as well.
I thought I was protecting them but, with hindsight, if I had asked for help then I wouldn’t have been so unwell. Over the course of a decade I was taken to A&E every six months with glucose levels so high that they became a medical emergency known as diabetic ketoacidosis.
It wasn’t until 2009 when I was lying on a hospital trolley in the resuscitation department that I knew I had gone too far.
Physically and emotionally, I felt worse than I ever had.
Something about this admission was different and for the first time since my diagnosis, I was scared.
Previously, the rebellious and independent character I had built was accustomed to feeling invincible.
However I was now terrified. I turned to my mum and asked: “Am I going to die?”
It was after that admission that my life changed for the better.
I decided to stop rebelling against my diabetes and to take control of it in the way I should have from the word go.
I knew that I couldn’t subject my body to high glucose levels any longer as the consequences would soon catch up with me.
Treatment For Diabetes (Photo: Getty)
I knew that I needed to make this change for myself and my family and I promised myself that I would become the strong, confident and empowered person that I am today.
The greatest tool that I used in order to regain control of my diabetes was the Diabetes Online Community – a group of patients, families and healthcare professionals who come together across many online platforms in order to support and educate one another.
This community opened my eyes to what was possible and what I could achieve in living a life with diabetes.
They taught me about the positives that came with living with this condition and, most importantly, they showed me that I was not alone.
The sense of belonging is a powerful feeling like no other.
As part of my self-prescribed diabetes rehab I decided to write about my experiences on Twitter – @ninjabetic1 – and in a blog called Ninjabetic, The Highs and Lows of a Ninjabetic Life.
Just a few years later I have over half a million readers, listening to me talk about my past experiences and my hopes for the future.
I started using an insulin pump along with the Freestyle Libre glucose monitoring system and I educated myself through a flexible and interactive online programme called BERTIE.
I became a patient advocate, working with sufferers in order to ensure the NHS is providing the best care it can in order to ensure people with diabetes live long happy and healthy lives.
I also became part of the NHS when I qualified this year as a nurse, vowing to one day assist in making the changes in diabetes care that patients and their families need.
My son was 22 months when he was diagnosed with type 1 diabetes. We have been through everything, from dealing with insulin pumps while wearing diapers to Valentine’s Day school parties and sleepovers. Now he is eleven years old and in middle school. He and I handle his diabetes every day.
Shari and her son Andrew
When he was five, he was invited to a birthday party. When I dropped him off, the mom said her husband was just leaving to go get the pizza. I decided to stay until the pizza arrived so I could dose him for the correct amount of carbohydrates. Needless to say, an hour and a half later, I felt incredibly awkward still being there and the pizza still hadn’t arrived. I found myself staying in the basement of the boy’s house with 20 little boys running around me having a nerf war. I was super annoyed and told myself, “Something has to give.” As I drove home, I realized I hadn’t stayed because the pizza hadn’t arrived, but I stayed because I was afraid to leave him alone at a parent’s house that didn’t know much about diabetes. He was at an age where it was awkward to helicopter around him, yet I didn’t trust his ability to make life and death decisions on his own. Choosing not to allow him to go to the party because of diabetes wasn’t an option to me. The next day, I went to the store and got my little man a flip phone. I was super uneasy about the judgement I would receive from other kindergarten parents. I knew it seemed ridiculous to give him a phone at such a young age. However, I decided when he was away from me, I needed to know that he was ok. Of course, he was thrilled with his new little piece of independence. We discussed rules and because it was only a flip phone, he couldn’t play games on it.
For the next six years, there were many times that I realized getting him that phone (and a couple of upgrades since then) was probably the best diabetes mom (or D Mom as so many of us love calling each other) decision I have ever made. I have been able to set rules about phones early when he still listened and followed them. He’s been able to learn responsibility for an expensive item (he never did find out that first flip phone was actually free when I added another line to our plan for $10.) To him, that phone was important and irreplaceable. It allowed him freedom. Having type 1 diabetes when you are growing up can be stifling enough. When you are nine and ten years old, you really don’t want your mom following you around the neighborhood, to a party or to a sleep over. He was able to do all of these things knowing that if he was in trouble, I was only a call or text away. More importantly, it allowed him to learn to trust himself.
I also imagined caring for your diabetes at a young age would be kind of like taking that first leap into the lake and knowing you would be able to keep yourself above the water. With each new opportunity of independence, he has handled himself responsibly. He understands that the phone is his way to care for himself.
Andrew with his phone
Finally, it allowed me freedom. When you are a D Mom, you are as protective as a mother bear in the wild. Every minute of the day and night, low blood sugars are ready and waiting to snatch your baby from your watch. We are vigilant and fearless and it is hard to let our cubs out of our sight. Knowing he had that phone, allowed me to go back to work. It allowed me to let him go to the sleepovers and allowed me to sleep while he was there. He still doesn’t know I am usually within ten minutes of him. It allows me to watch him learn to care for himself and teach him pitfalls and dangers along the way.
Getting him a phone was a great decision for our family. Every family is different and every child has their own needs. For our family, the phone gave us many opportunities for him (and me) to have a little independence while still feeling connected. And I don’t regret it.
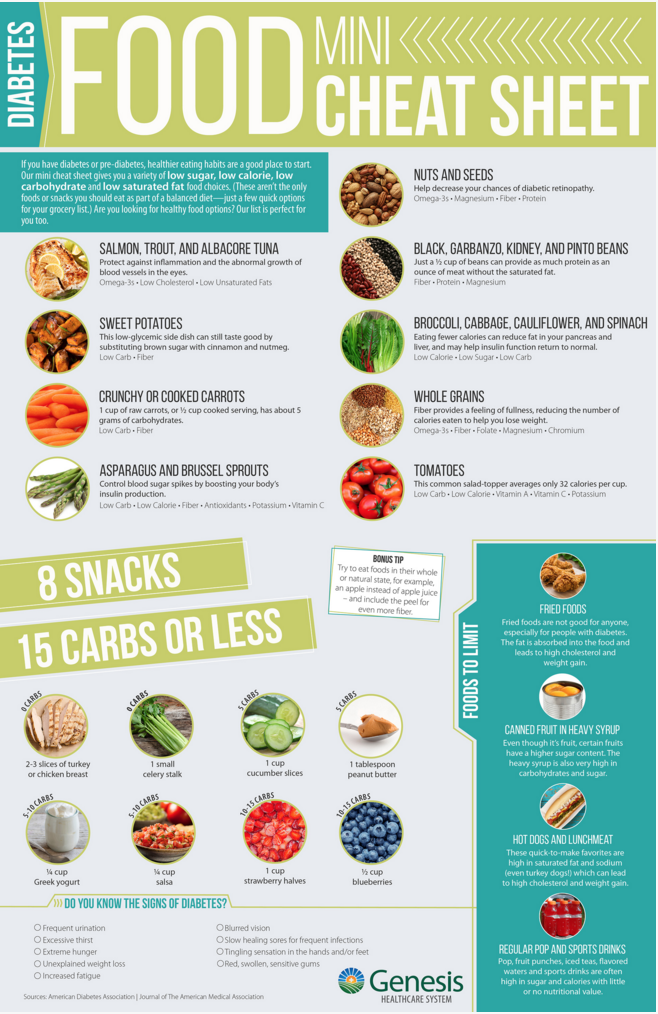
Genesis Healthcare System of Zanesville, Ohio put together this helpful Diabetes Food Cheat Sheet!
If you have diabetes or pre-diabetes, healthier eating habits are a good place to start. Our mini cheat sheet gives you a variety of low sugar, low calorie, low carbohydrate and low saturated fat food choices. (These aren’t the only foods or snacks you should eat as part of a balanced diet—just a few quick options for your grocery list.) Are you just looking for healthy food options? Our list is perfect for you too. ➔ Download the Diabetes Food Cheat Sheet (PDF)
medwireNews: Researchers say that physicians should be alert for worsening depression in patients with type 1 diabetes, after finding it to be associated with poor metabolic control.
“While depressive symptoms themselves require therapy, they also contribute negatively to diabetes-related medical, social and psychological outcomes, and therefore need to be addressed,”writes the team in Diabetologia.
The team identified three trajectories of depressive symptoms, measured on the Symptom Checklist 90-R (SCL-90-R), among 313 patients, aged 28 years on average, 258 of whom participated in all five annual follow-up assessments.
Patients in the first trajectory – 79.9% of all patients – had no depressive symptoms at any time. A further 6.4% of patients were in a second trajectory; they had gender-adjusted T scores for depressive symptoms that were close to the threshold for clinical depression at baseline, worsened over the next 2 years, but then improved.
The 13.7% of patients in the third trajectory had baseline T scores indicative of depression (average 61.4), and these worsened further during follow-up, to an average 5-year score of 73.8. By this point, these patients had significantly poorer glycemic control than those in the other two groups, with glycated hemoglobin scores of 8.2% versus 7.2%, despite no differences between them at the 1-year follow-up.
These patients also had worse diabetes-related quality of life for strain, strain related to blood glucose levels, and satisfaction, compared with patients without depressive symptoms. They had higher levels of diabetes-related distress and perceived that they had less family support.
“Clinicians may benefit from this knowledge,” say Hanna Kampling (University of Freiburg, Germany) and co-researchers, suggesting that diabetes patients should undergo routine screening for depression, with referral for treatment when necessary.
The researchers note that although the burden of diabetes was high in some patients, it nevertheless affected a relatively small proportion of the patients.
“This is surprising, as one would expect that a disease with lifelong implications in terms of medication and lifestyle, and with a potential risk of secondary complications, would have a stronger impact,” they say.
However, they add that the baseline rate of major depression according to DSM-IV, at 5.8%, was more than double that reported in people without diabetes, and depression worsened over time in around 14% of the whole cohort.


 She is my furry shadow, my best friend, and I can’t see my life without her.
She is my furry shadow, my best friend, and I can’t see my life without her.


 In the middle of the night, Luke’s levels dropped extremely low, and as he was trained to do, Jedi woke Luke’s parents to let them know.
In the middle of the night, Luke’s levels dropped extremely low, and as he was trained to do, Jedi woke Luke’s parents to let them know.

 On the flip side, some of the things we often do to provide emotional support are generally seen as unhelpful. Here are some things to avoid:
On the flip side, some of the things we often do to provide emotional support are generally seen as unhelpful. Here are some things to avoid:
 It offers a description of what a diabetes educator does and the role they can take when trying to navigate care of a child in the school setting. This is the part of the article that I thought might be the most helpful for parents to know. From the, admittedly very few parents I have talked to, I’m not sure that people are using diabetes educators in this way. The article says that a diabetes educator can (p.35, direct quote):
It offers a description of what a diabetes educator does and the role they can take when trying to navigate care of a child in the school setting. This is the part of the article that I thought might be the most helpful for parents to know. From the, admittedly very few parents I have talked to, I’m not sure that people are using diabetes educators in this way. The article says that a diabetes educator can (p.35, direct quote):